Web 3.0 decentralised health - achieving better health by uniting stakeholders in online Communities.
Health is a human right, that the inequalities in existing health status are ‘politically, socially and economically unacceptable’ and that essential health care must be made ‘accessible to individuals and families in the community through their full participation’ (1)
Contents
2.0 The problem: An unsustainable Illness Economy and fragmented health ecosystem. 4
3.1 Empowering people through ‘Patient Activation’ and ‘Supported Self Management’ 5
3.2 Aligning health Stakeholders to incentivise Patient Activation via Communities. 5
5.0 Web3 for health promotion. 8
5.1 Decentralised token economy and its value to health 8
5.3 Token Staking to DAOs, TVL and Token burn. 12
5.4 Trust-less Community DAO Validation 13
5.5.3 Token allocation (team, investors, community) 17
5.7.1 Regulatory compliance 17
7.2 Clinical leaders for communities. 23
7.3 Key opinion leaders to promote tokenisation 23
Tokenisation offers an ideal solution to align all health stakeholders into a web 3.0 decentralised economy.
Healthcare costs associated with treating an ever-increasing burden of complications from chronic diseases grow unrelentingly and are unsustainable. Leading healthcare organisations including the NHS and WHO support the use of 'patient activation' and 'supported self management' in order to turn this tide. Patient activation through ‘Communities of Practice’ empowers people to become more engaged with their health, making better health choices resulting in better health, earlier treatment of illness and less cost.
Tokenisation of Patient Activation through online Communities of Practice results in a win-win scenario for all stakeholders in population health. The Health-Shared token offers a unique opportunity to establish a decentralised solution with landscape shaping potential in health.
The opening statement of this document is the 1978 call for community participation - the
Alma Ata declaration by the WHO. Legacy activity to address this right involved training Community health workers modelled on China’s ‘Barefoot Doctors’. In theory, they acted as community ‘change agents’ who would make an impact on poor health behaviours and ‘empower’ communities to make joint decisions about health care (2).
Today’s world is digitally connected but physically fractured. Web3 digital health offers a far reaching and cost effective potential to achieve the ambitions of the 1978 declaration.
Population ageing is endemic in developed countries. By 2050 the number of persons over 60 years is expected to double, from 901 million to nearly 2.1 billion (3). This puts pressure on health systems, increasing the demand for care, services, and technologies to prevent and treat noncommunicable diseases and chronic conditions associated with old age. Chronic noncommunicable diseases are responsible for 68 % of world's deaths (4) and account for over 70 % of healthcare spending in the US and European Union (5,6). Approximately 15 million people in England are living with a chronic condition (7), significantly impacting health-related quality of life (8).
The healthcare sector has a major impact on national economies, accounting, in the European Union, for 10 % of GDP and 8% of the total workforce. UK healthcare costs have increased dramatically over the 21st century from £78.9 billion in 2000 to £269.5 billion in 2020 (9). Policymakers including the EU have made statements like "the need to make health systems sustainable by making them more effective, accessible and resilient has been duly recognised by policy-makers at the EU and national level" (10).
15 chronic conditions will cost the Global health economy $371 billion over the next 15 years (11,12)). These 15 chronic conditions account for 80% of total healthcare spending (4). The drivers behind these conditions are 8 health related behaviours (4): smoking, alcohol consumption, physical inactivity, poor diet, poor adherence, poor stress management, insufficient sleep, and lack of health screening. Adhering to just 4 healthy behaviours has been shown to reduce the risk of developing type 2 diabetes by 93% and risk of having a myocardial infarction by 81% (13) .
In order to re-focus on a 'prevention is better than cure' paradigm and empowering patients to self-care the currently siloed multiple stakeholders in the health journey need to work together.
Stakeholders include:
Collaboration between stakeholders currently lacks structure (15). Collaboration, if achieved can have a potential ‘fly-wheel’ effect and improve outcomes whilst constraining costs (16).
Tokenisation has previously been used to incentivise patients into ‘rewardable actions’ (17). The size of the token reward was found to correlate with the likelihood of a user allowing access to their health information. Token rewards have been shown to relate to a three fold increase in adherence to activities of daily living (18) and also to participate in clinical trials in a simulation study (17).
'Patient activation' and 'Supported self-management' have the potential to promote better health and Quality of Life (QoL) outcomes through empowering individuals. The WHO defines patient empowerment as ‘a process through which people gain greater control over decisions and actions affecting their health’ (19), and is a priority area to improve healthcare outcomes (20).
Patient activation and increased capacity to self manage can be promoted by Cognitive Behavioral Therapy or motivational interview approaches, but these strategies do not scale and are prohibitively expensive.
Patient activation can be improved with other strategies i.e. using an online health record resulted in patients having higher rates of adherence to medication (21). Adhering to just four healthy behaviours has been shown to reduce the risk of developing type 2 diabetes by 93% and risk of having a myocardial infarction by 81% (12).
The patient activation measure (PAM-13) is a 13-item questionnaire that has been used in over 700 peer-reviewed publications and is a well validated measurement tool which we intend to use as an indicator of patient empowerment. Higher PAM scores are associated with increased health promoting behaviour, such as regular check-ups, healthy diet, and regular exercise as well as reduced health-damaging behaviour such as smoking and illicit drug use (22). These are corroborated by lower body mass index scores, HbA1c levels, blood pressure, and cholesterol readings. Furthermore, PAM scores are predictive of the next year’s healthcare costs, with those with lower scores having significantly higher costs (19). Importantly, PAM scores can be impacted by interventions, with changes ranging from 2.5 to 6.5 on the 100-point scale (19).
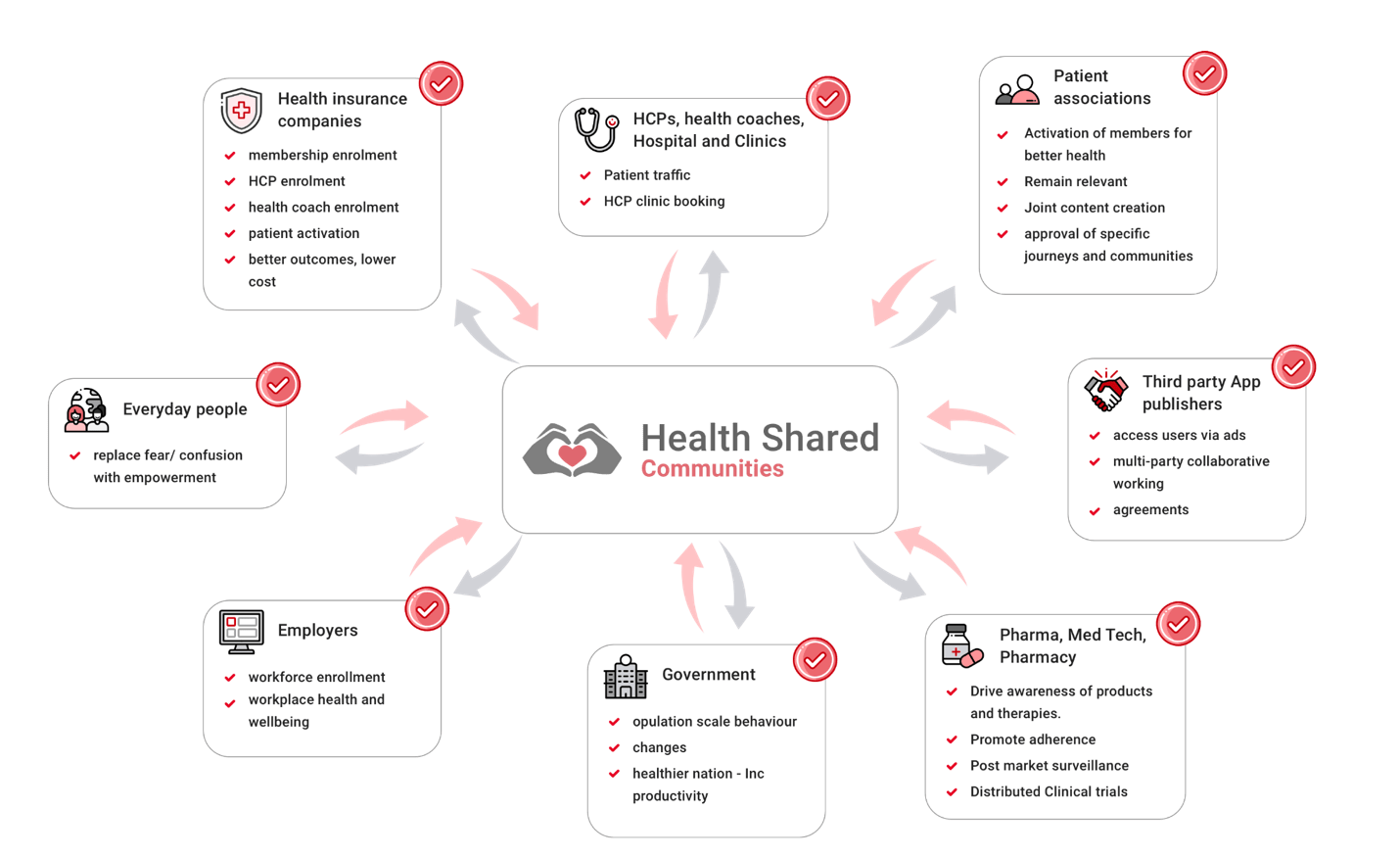
Achieving patient activation is in the interests of all stakeholders in the health.
Communities of practice (CoPs) are groups of people who share a concern, a set of problems, or a passion about a topic, and who deepen their knowledge and expertise by interacting on an ongoing basis (23). Online CoPs are increasingly recognised as a key enabler of better self-management by WHO and the NHS (24,25). Health-Shared communities empower people to ‘patient activation’ through the optimised functioning of online Communities of Practice.
Figure 1. All stakeholders in the health journey benefit from patient activation.
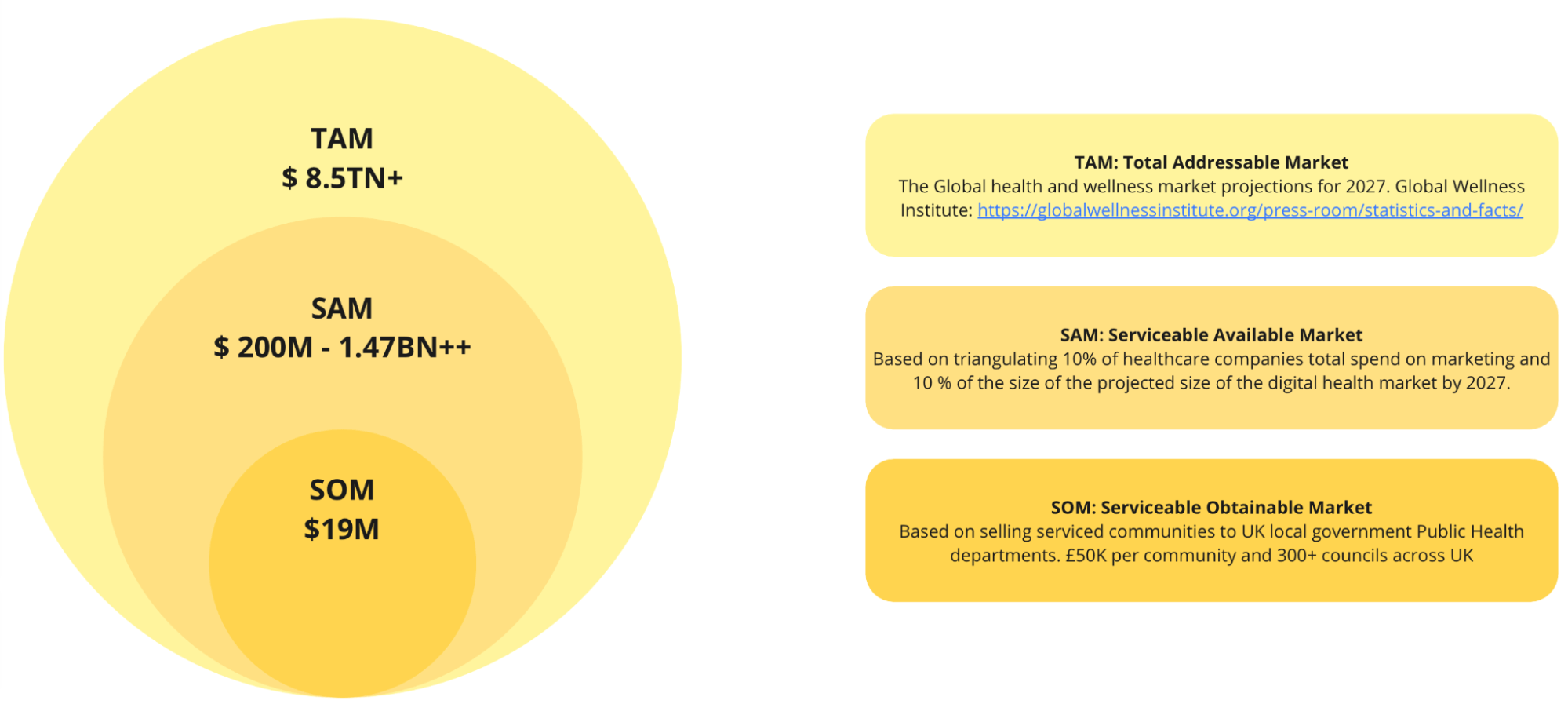
The Global Health and Wellness economy is projected to cost £8.5 trillion by 2027 (38).
Figure 2. SOM, SAM and TAM for Health-Shared.
The total revenue for 2,193 healthcare companies listed on Reuters Aggregates reports is $1.89 trillion for LTM (26). 90% of listed companies have revenue ranging $10 million to $1 billion. Healthcare marketing budgets average 10% of revenue (27). This roughly equates to $2Bn. We assume that we can capture 10% of these budgets equating to 200M from industry alone. The Digital Therapeutics market has been projected to be worth $14.7B by 2027 with a CAGR >21% (28). This translates to a Serviceable Available Market of between $200M and $1.47Bn.
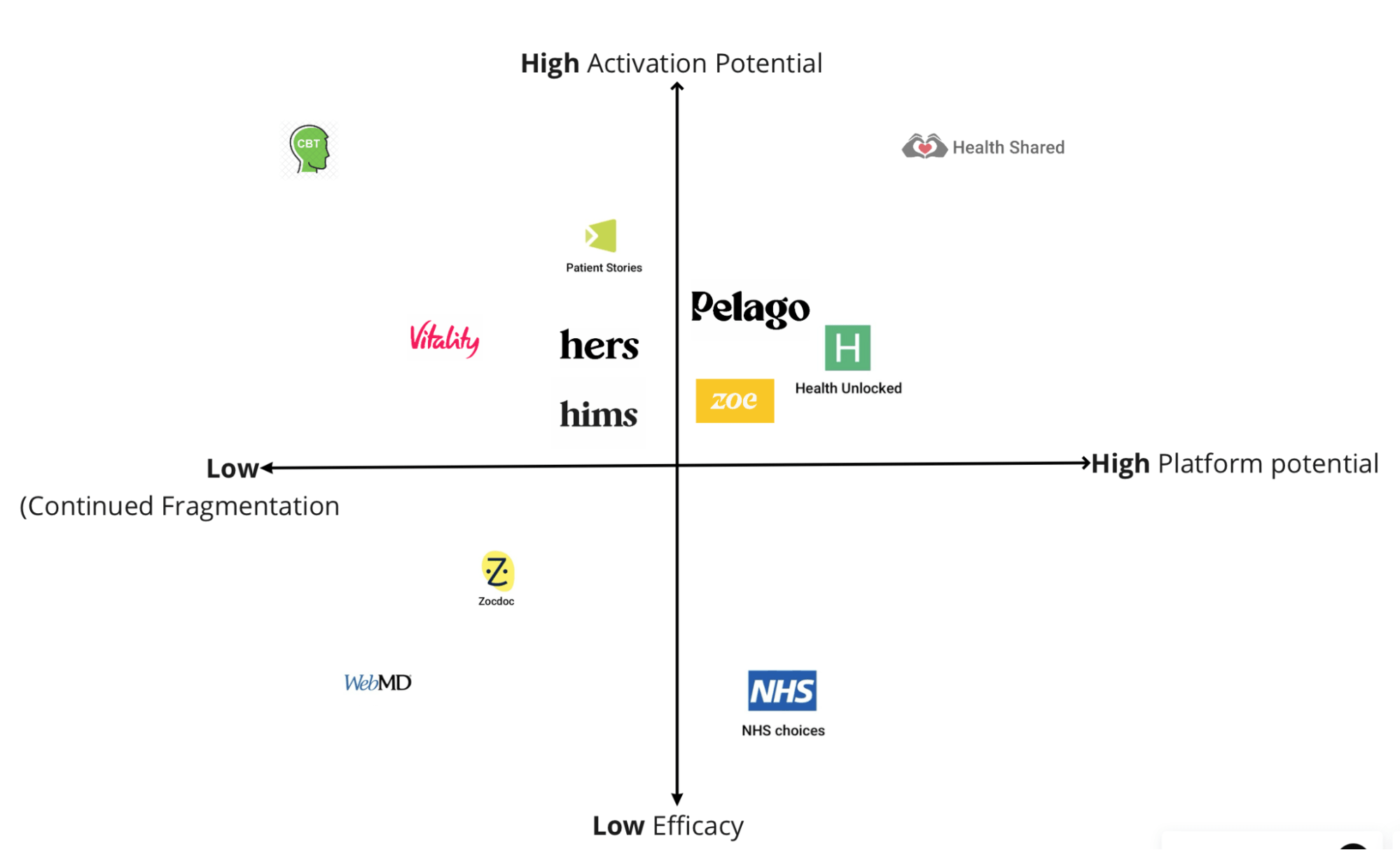
The patient activation space is becoming more crowded with multiple entrants. Most fall into well defined categories including online Cognitive Behaviour Therapy/ Motivational Interviewing; Condition/ persona specific ‘personalised’ solutions; Online content sites; Activity gamification and patient communities. The critical dimensions to achieving better health outcomes, better quality of life and lower cost to society involve patient activation capability and scalability with platform economics. Typical market competitors are illustrated below.
Figure 3. Competitor analysis for potential solutions to transform from an illness to a health activation economy.
A decentralised web3 approach solves some of the core problems with the health ecosystem, namely, its fragmentation and the misaligned interests of key stakeholders. Tokenisation can align all health stakeholders to promote Patient Activation resulting in positive behaviour change at population scale. Communities function as a common mechanism through which multiple stakeholders can collaborate.
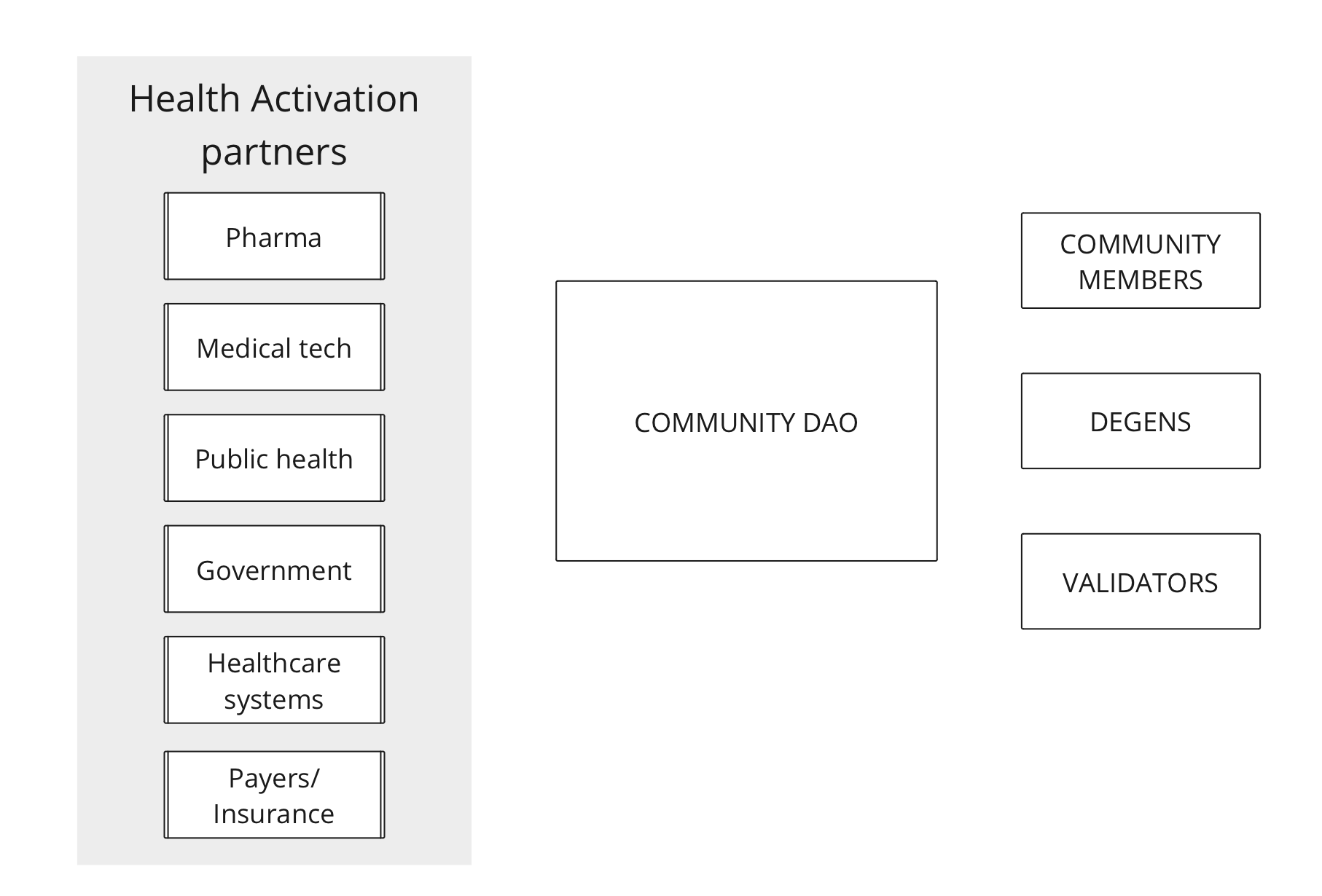
The benefits stakeholders gain and hence the reasons to align and participate in Health-Shared communities can vary according to the stakeholder and have been enumerated in section 3.2. The Health-Shared token economy consists of the health stakeholders mentioned above as well as Degens and Validators. In this ecosystem, ‘health stakeholders’ are essentially Health Activation Partners.
Figure 4. Components of the Health-Shared token economy.
Stakeholder/ Activation partners and Community members’ motives have been described above. The remaining three components have essential functions:
An overall schema for functioning of the Health-Shared token economy and how it incentivises all component parts of the health ecosystem is described below.
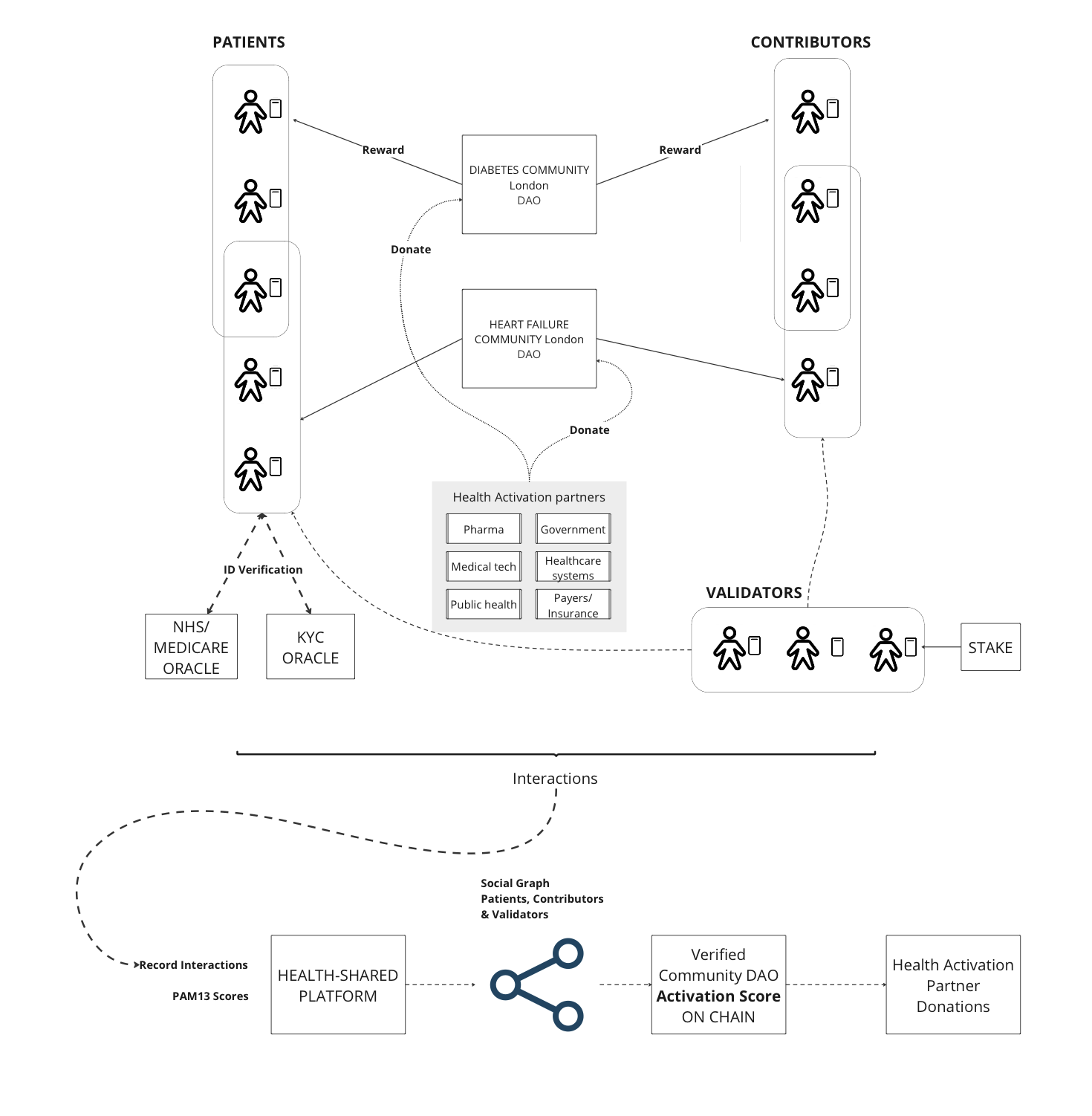
Figure 5. How component parts of the Health-Shared ecosystem interact to achieve population scale Patient Activation.
Community DAOs are linked to territories but not necessarily exclusively. Multiple communities dealing with similar issues can occupy the same or overlapping territories and can serve differing groups. Positive interactions between content contributors and consumers are rewarded by Community DAOs. Health-shared users are free to join any number of Community DAOs. Validation of Community members is done via Oracles or KYC mechanisms, social graph analysis in conjunction with face to face Validators who in return for Staking and the work they perform receive a yield.
Community DAOs with verified members generate an activation score for the Community DAO which is visible to Health Activation partners who can donate to relevant community DAOs to amplify their effect.
A simplified token flow is described below. It begins with community DAOs issuing tokens to community members as a reward for interacting in the community and creating content.
Other stakeholders can purchase tokens from an exchange to be used to augment the community token reward allocations. The interaction between directly community earned tokens and stakeholder supplemented incentivisation is shown in the figure below.
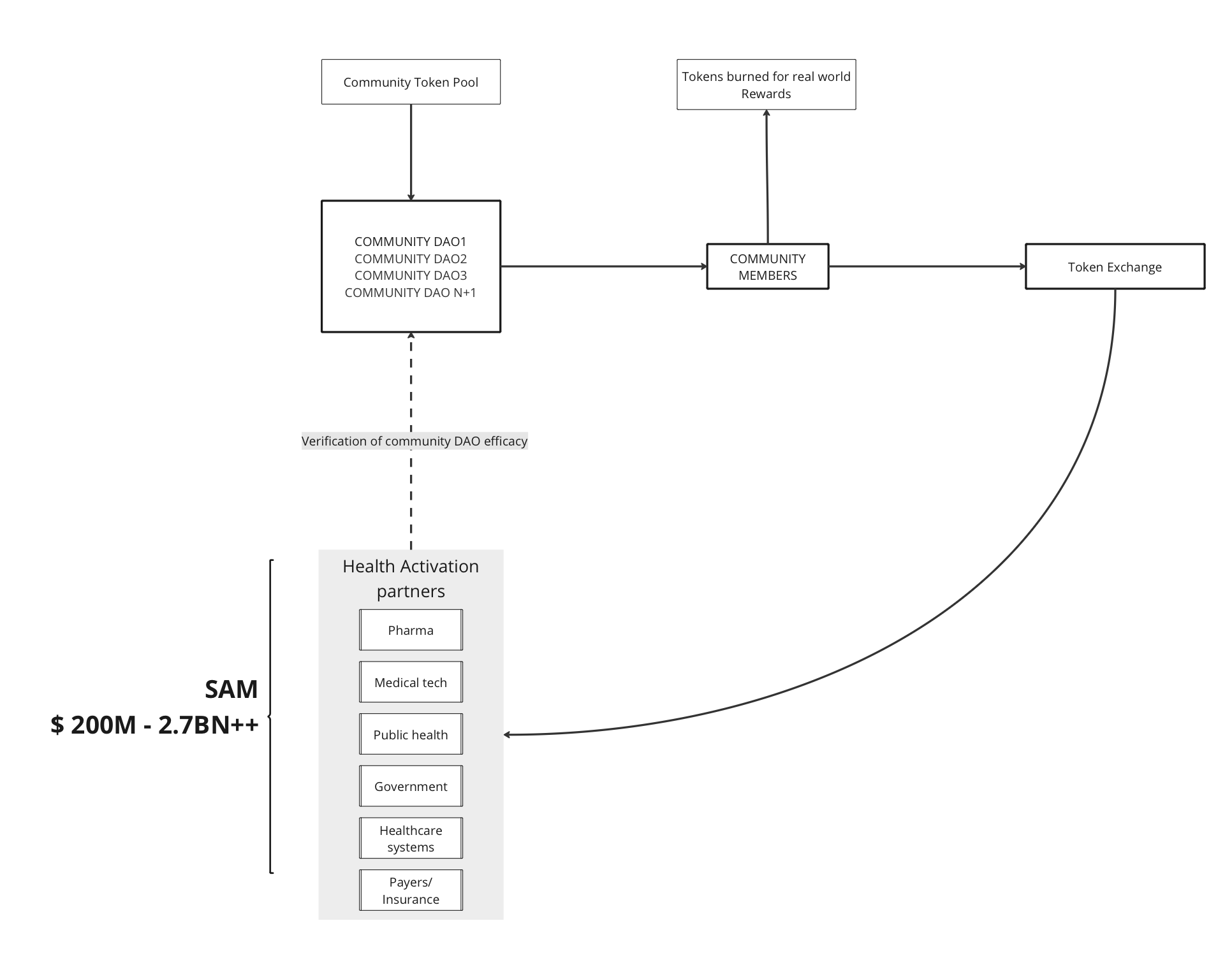
Figure 6. Flowchart demonstrating token flow. Demonstrating how Industry will incentivise DAO community activation activities by purchasing and distributing tokens via Community DAOs.
Community member tokens holders can choose to hold tokens for appreciation over time, or redeem them for real world rewards. Real world rewards are a way of, for instance, incentivising community members to interact and support communities locally. The local nature of the real world rewards are highly aligned to incentivise local people to act for their local communities. Redemption of tokens for real world rewards will result in tokens being burned and lost to the general pool.
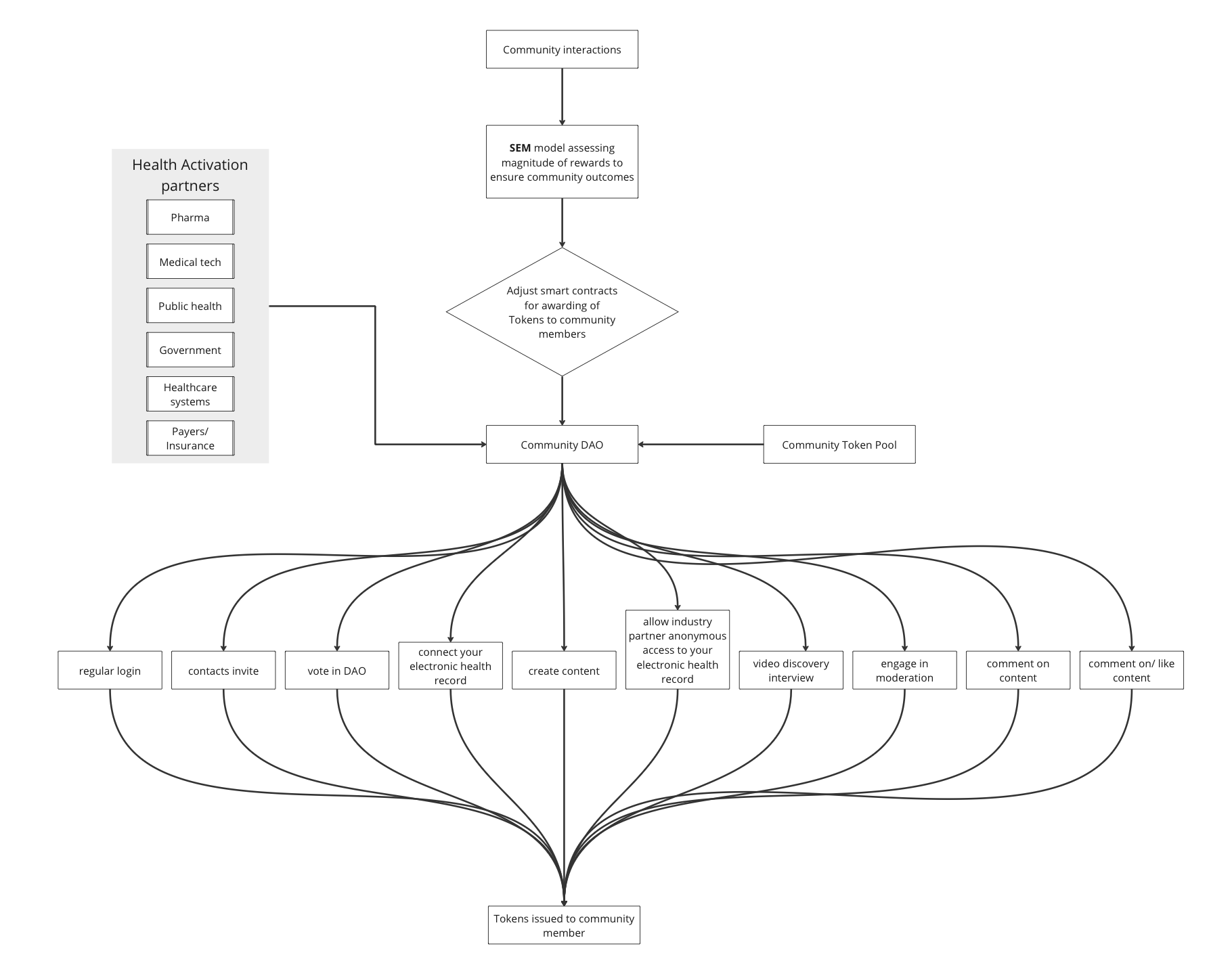
Community DAOs will reward community members for engaging in a number of activities which are beneficial to community effectiveness. The magnitude of these rewards is determined by inference from the community Systemic Equation Model, designed to optimise community performance. This is described in the figure below. Identification of individuals in the community who are more likely to contribute has also been established (29). Such individuals can potentially be targeted for incentivisation.
Figure 7. Flowchart demonstrating confluence of ‘earned’ tokens for rewardable community activities and ‘supplemented’ tokens issued via health activation partners.
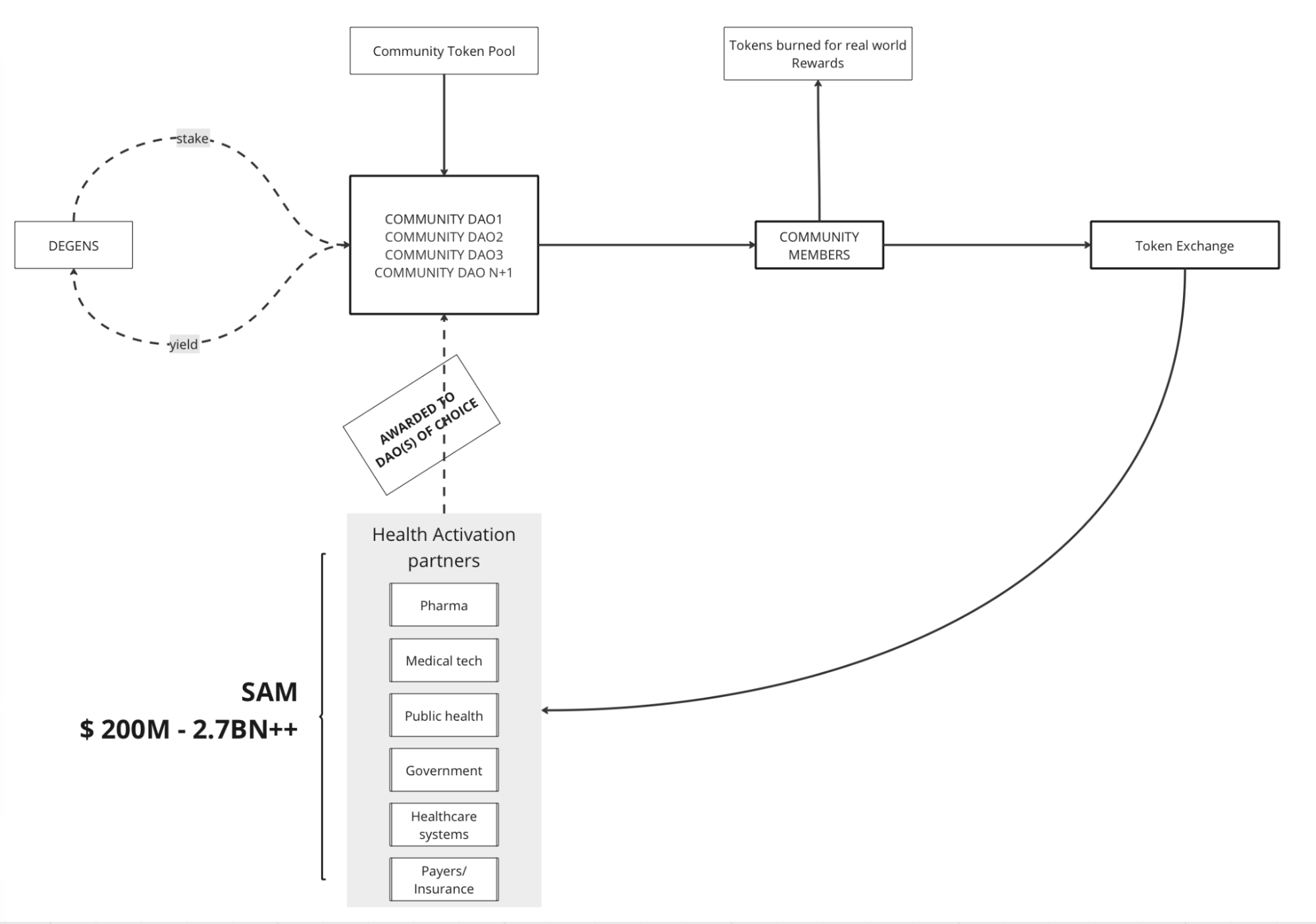
Once the community model is established, community DAOs will be encouraged to act autonomously. They can raise capital in the form of tokens from Degen investors. They can use this capital to engage in activation activities including curating and creating content and rewarding community activism. They can earn an income from stakeholder (industry and government partners) awards to support activation. After covering administration costs, they will disburse excess tokens to Degen investors as yield.
Investors can choose to stake DAOs based on their community activation metrics for a yield on the staked tokens. This staking mechanism will result in a percentage total value lock.
Community members who have earned tokens can redeem them for real world benefits provided by activation partners or reward networks. Redemption of tokens results in token burn. The combination of TVL and token burn creates deflationary pressure.
Figure 8. Flow chart demonstrating Degen staking, yield and resulting total value lock.
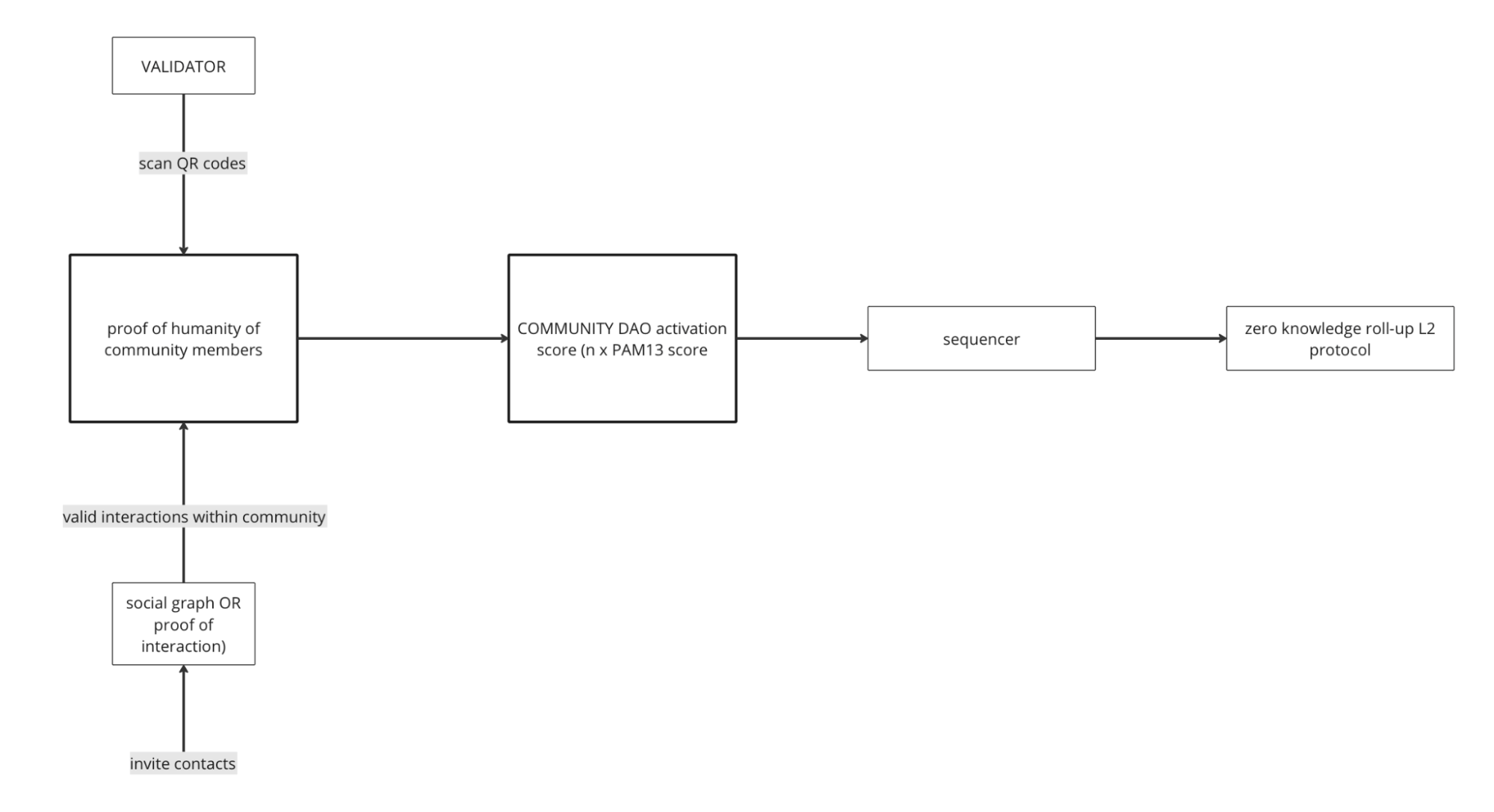
Activation partners require assurance that the Community DAOs are achieving the desired common goal. This requires two objectives being met. The first is proof of humanity for community members and the second is to validate that the community DAOs are achieving measurable activation (PAM13 score). Below is a schema to achieve these aims.
Figure 9. Flowchart demonstrating Community DAO validation.
Proof of humanity can be achieved by using Social Graphs in conjunction with verification by Validators based in territories who can prove a sample of community members are real humans through face to face interaction. Proof of humanity can also be corroborated using Oracles ie in the UK, the National Health Service has a verification scheme which can be accessed via API call.
Proof of effectiveness of Community DAOs should be via measurable and verifiable patient reported outcomes metrics (PROMS) - namely increment in the PAM13 score. Both sides of this assurance are measurable and verifiable and reportable to a sequencer who will report using a zero-knowledge roll up protocol.
With these two aspects assured, activation partners can invest into DAOs with confidence in their investment. Ultimately all validation functions will be processed programmatically on chain.
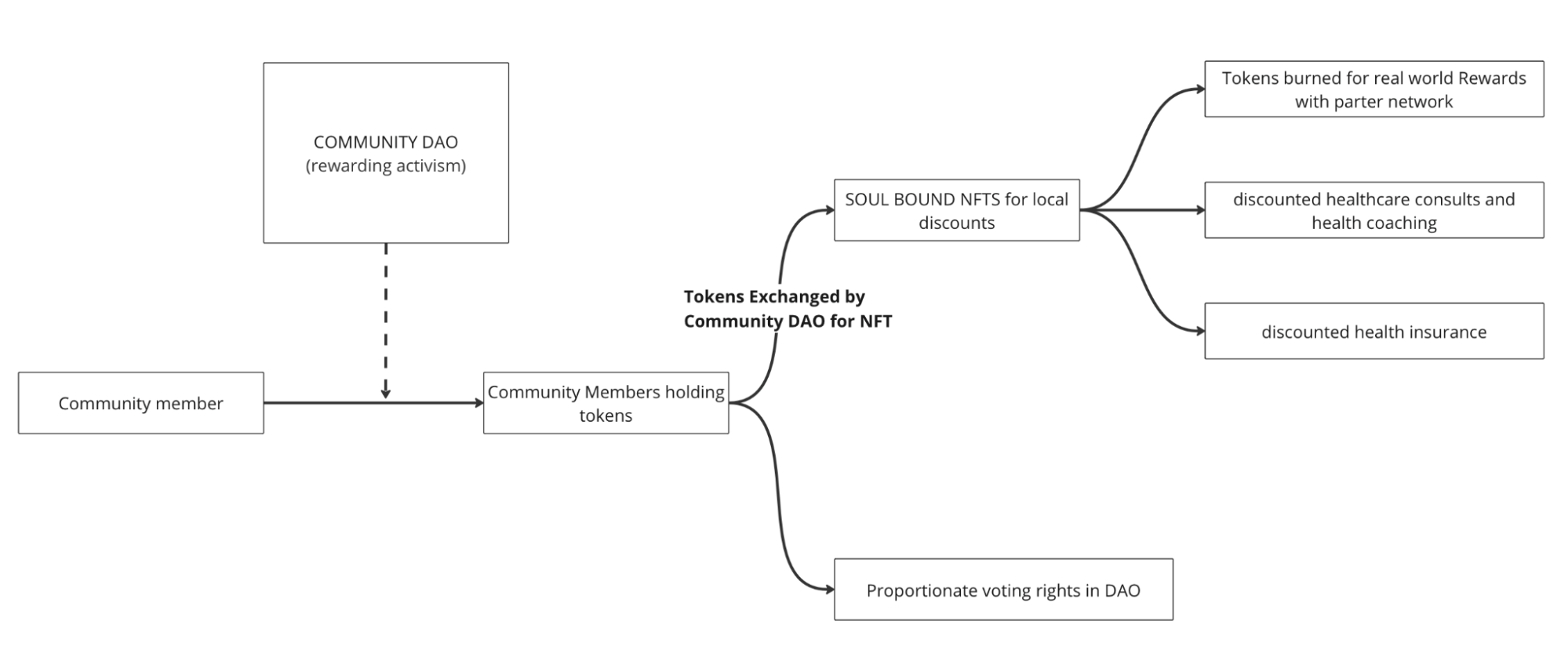
The utility to stakeholders can be seen in four categories:
Relevant health stakeholders can purchase tokens to disburse to community members who have earned tokens through community activity.
Tokens can be redeemed for rewards via local Community DAOs ( in partnership with government or other partner organisations, eg gym memberships/ healthy lifestyle services discounts, health coaching, health insurance etc). Tokens redeemed for these rewards will be exchanged for Soul Bound NFTs by local Community DAOs. These NFTS can then be used. This will result in token burn.
Communities will act as DAOs. In order to have voting rights, community members must possess tokens. Representation of community members will be dependent on the amount of tokens held.
This is demonstrated in the figure below.
Figure 10. Flowchart demonstrating token utility.
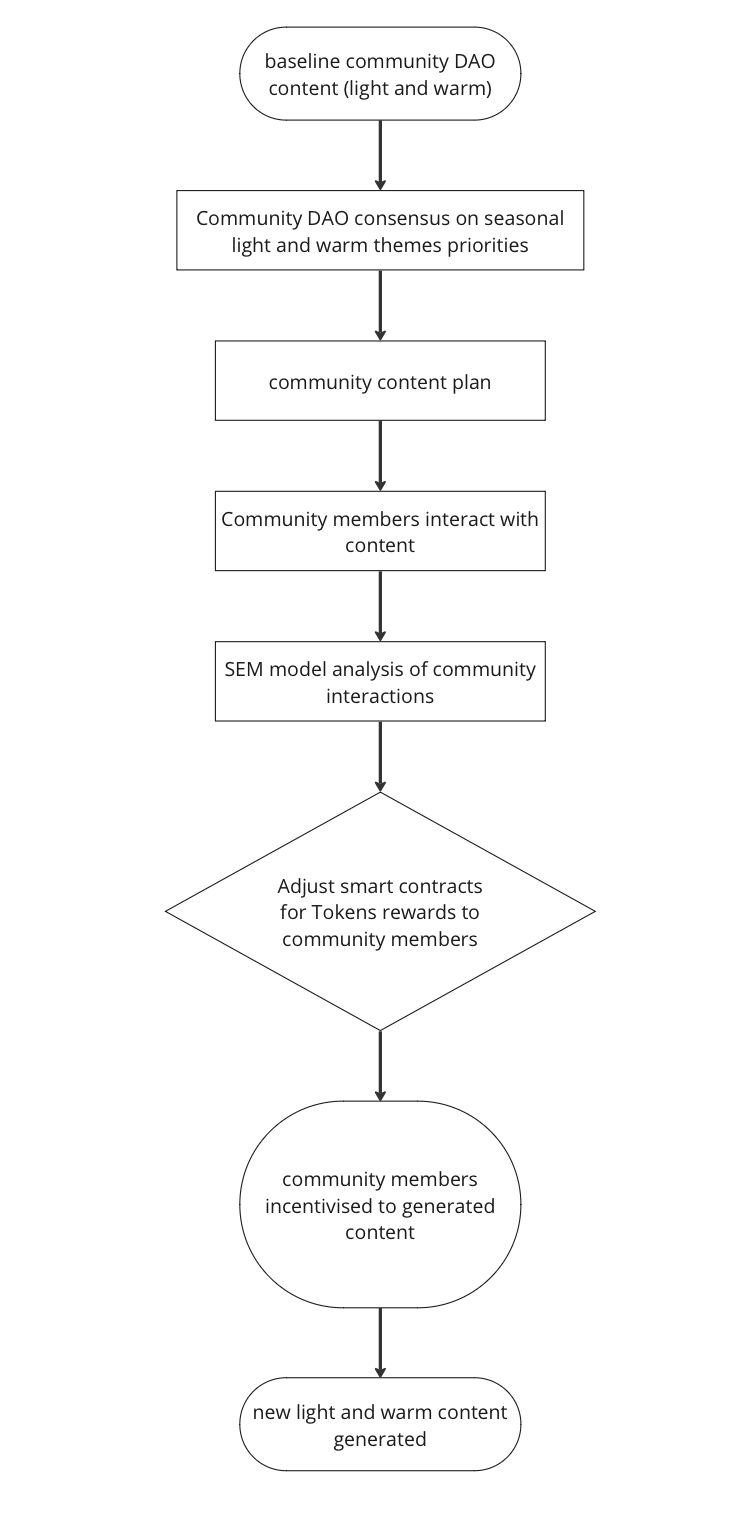
The Structural Equation Model (SEM) analysing community interaction data will ascertain which aspects of community activity need to be incentivised at higher levels to maintain optimum community functioning. These outputs will adjust smart contract parameters which issue token rewards to community members.
The role of the SEM analysis inputting into smart contracts which issue tokens to community members is demonstrated in the figure below.
Figure 11. Interaction between Structural Equation Model of factors affecting community outcomes and community DAO. This cycle ensures that there is continuous real world monitoring and adjustment to optimise community outcomes.
The Health Coin will be an ERC-20 Token.
Token supply will be deflationary. As the Health-Shared ecosystem grows, less incentivisation will be required for community members to create, share, invite, moderate etc and hence token supply will become harder.
The Tokens will be minted and initially distributed through a Token Generation Event.
|
Recipient |
Allocation |
Unlock Cliff |
Post Cliff Vesting |
|
Public sale |
4% |
0 months |
12 months |
|
Community reserve |
58% |
0 months |
60 months |
|
Pre-seed investors |
5% |
3 months |
24 months |
|
Strategic investors |
8% |
3 months |
36 months |
|
Core team |
22% |
12 months |
48 months |
|
Token advisors |
2.5% |
12 months |
24 months |
|
Global ambassadors |
0.50% |
12 months |
36 months |
Tokens will be disbursed through a TGE.
We are compliant with region specific pharma and med tech codes of conduct and have a robust governance structure in place. Health-Shared is governed by a charter and oversight is through the board, an external governance advisory board and a clinical advisory group made up of recognised experts in their respective fields.
We will need to reserve a liquidity pool of tokens to be deployed responsively to maintain market liquidity.
Health-Shared platform is operational as is the ability to analyse and categorise content into light (explicit) and warm (content). We have a proven track record of being able to deliver technological solutions include the systemic equation model and the psychographics ML model. Token aspects will be managed and delivered by Ten, our blockchain partners.
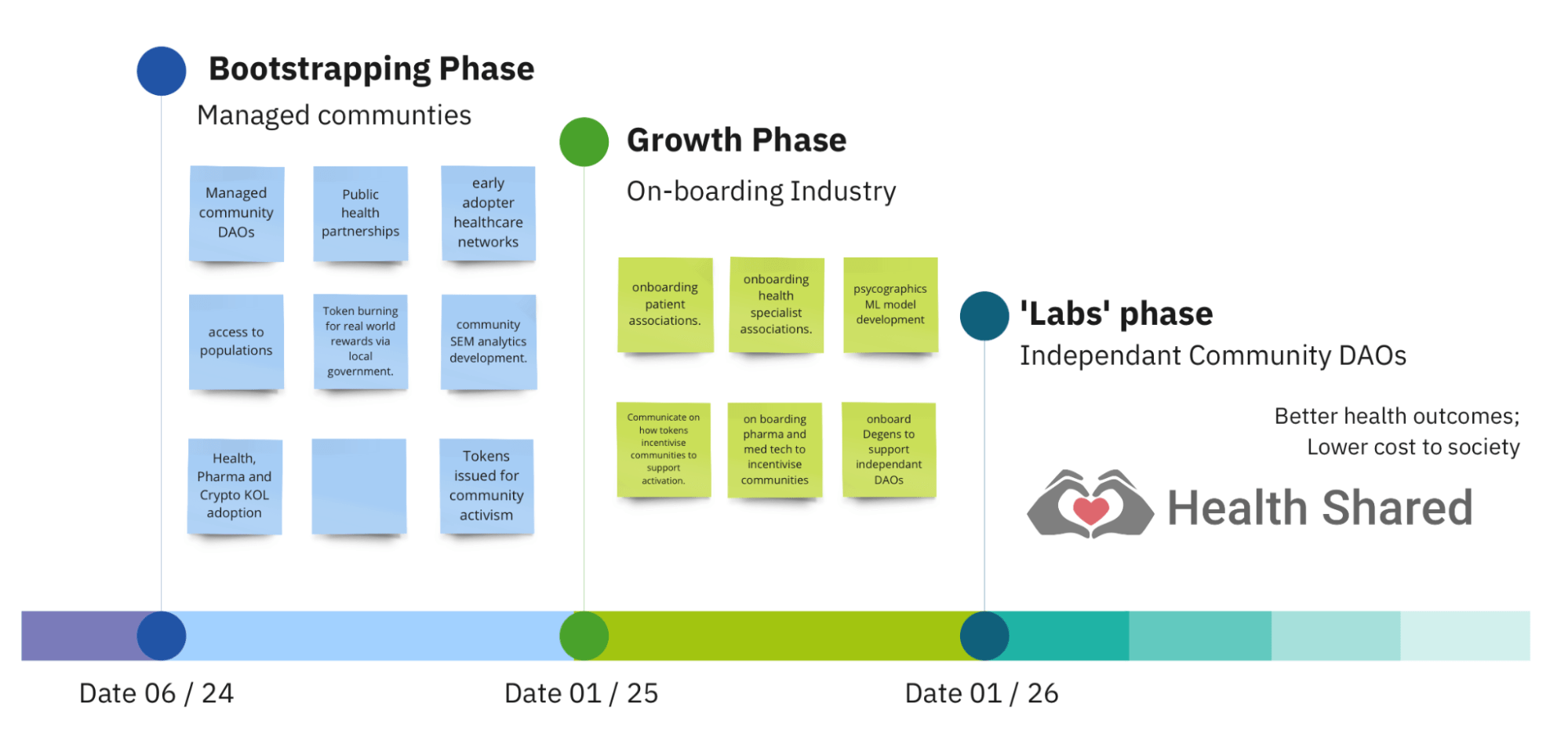
Health-Shared has identified three phases in establishing fully functional tokenised communities with measurable population scale patient activation improvement. The strategy adopted is of ‘inverting the sales funnel’ (49). This relates to a B2B strategy rather than a B2C. The stakeholders we are partnering with are natural early adopters and have access to the population at large. Hence they represent our ‘entry wedge’ into the market at large.
The route to market roadmap consists of:
Figure 12. Product roadmap showing key milestones.
In this phase, all community DAOs will be created and managed by Health-Shared on behalf of partners. This phase is currently seeking partnerships with local government public health departments. Contracts are undertaken to establish and run local communities for specific conditions which are priorities for the local government. Our pilot community is ‘Diabetes and Weight Management’ in the London Borough of Kensington and Chelsea. Through the Borough infrastructure, we will reach all residents who this community is relevant to or who may be interested or have affected friends or family. This is estimated to be around 30-40,000 people in a population of 170,000.
We are also partnering with other early adopter organisations including healthcare networks who are paid according to a capitation model and are heavily incentivised to reduce the burden of illness. We are in early discussions with a large US healthcare network in the state of Maryland for this.
In this phase, the tokens will be issued for community activism and burned on redemption of local government sponsored health promotion and healthy eating offers. No open trading will occur and corporate buying will not be promoted.
Communications will be focussed around the benefits of communities and the ‘paying it forward’ recognition of early community members. Key opinion leaders who span industry and healthcare will be recruited to be ambassadors for the value proposition that Health-Shared offers. These ambassadors will co-create regular pieces of content to lay the foundation of the growth phase. We will also promote the patient activation activities we are co-delivering with local government public health departments to attract new partnerships.
In this phase we will be widening our outreach to large healthcare organisations as the bootstrapping phase will have lowered the barrier for these organisations to engage. This phase will also include partnering with organisations who will be keen to access the audience we have built in the bootstrapping phase including specialist societies and patient associations.
We may develop and deploy analytics systems to be able to identify individuals who are relevant to industry stakeholders in an anonymous manner and increase the number of tokens they earn from community activism.
We will publicise the successes of the bootstrapping phase and begin to talk about how tokens incentivise communities to activate everyday people.
In the ‘labs’ phase, health-shared will no longer need to manage all communities centrally as the token incentivisation mechanisms will be in place to facilitate Community DAOs to function. We will engage with pharma and medical technology companies with the proposition of facilitating them to activate everyday people relevant to conditions they would like to support.
Tokens will be listed on exchanges. The pharmaceutical and medical technology industry will be facilitated in purchasing and disbursing incentive tokens to relevant Health-Shared users.
A change in communications to tokens being critical to mass, population scale patient activation.
Prof Usman Jaffer
CEO
Usman Jaffer is a Consultant Vascular Surgeon and academic. Usman founded health-shared as a result of lived experiences.
Carl Dempsey
Chief Strategy Officer
Carl and Usman met over a health encounter. Carl immediately felt drawn to support the benefit health-shared has to offer to the world. Carl has over 20 years of senior board level leadership at J&J dealing with strategic partnerships.
Nikolai Matiushev
CHIEF TECHNICAL OFFICER
Nikolai Matiushev is a senior polyglot software developer. Nikolai has 20+ years of experience spanning multiple industries from mobile, embedded and web development to enterprise systems at major investment banks and hedge funds.
Nikolai holds MSc degree in Applied Mathematics and Physics from Moscow Institute of Physics and Technology (National Research University)
Dr Sadie Syed
Director of Content
Dr Sadie Syed is a Consultant Anaesthetist at Imperial College London and Director of Simulation and also leads the ‘How Our Teams Transform Program’ at Imperial.
Arif Minhas
Head, Strategic Partnership
Arif’s experience spans nearly 20 years in new business development and strategic partnerships with a strong trans-Atlantic & pan-European focus, He was also formerly part of Charing Cross Symposium.
Prof Usman Khan
Non-exec Director
Usman Khan is a past executive chair of the European patient forum. He is chair of the Motor Neuron Disease Association and is a public health expert. He has had multiple roles in the patient associations as well as health policy and governance.
We have a stong team of clinical leaders to manage clinical issues related to communities.
We have KOLs in the wings, ready to go.
Professor Nadey Hakim
Head of KOL relationships
Professor Hakim is a world renowned transplant surgeon and past Vice president of the Royal Society of Medicine. He holds numerous positions on various boards and organisations and is International relations lead at the Cleveland Clinic London.
Our development team is five members strong and has a proven track record of delivering complex technical solutions.
Ben Szubert
Machine Learning Engineer
Ben has worked at a number of health startups and has been co-author on our tensor decomposition paper. He has also helped set up our psychographics pipeline.
Cain Clark
Statistician
Cain is associate professor in statistics at the University of Birmingham and has an interest in Systemic Equation Modelling which is important to the underlying monitoring of community function and prioritisation of token allocation for community activism.
Ten is a Layer 2 rollup that hyper-scales and encrypts Ethereum. Ten allows Ethereum smart contracts to contain both public and private elements without changing the user or developer experience. Ten is supporting this TGE.
1. Report of the International Conference on Primary Health Care, Alma-Ata, USSR, [Internet]. WHO; 1978. Available from: https://www.who.int/publications/i/item/9241800011
2. Nations U. Department of Economic and Social Affairs. Popul Div [Internet]. 2015 [cited 2024 Jan 13]; Available from: https://www.un.org/en/development/desa/policy/wess/wess_archive/1967wes_part2.pdf
3. Organization WH. Global status report on noncommunicable diseases 2014 [Internet]. World Health Organization; 2014 [cited 2024 Jan 13]. Available from: https://apps.who.int/iris/bitstream/handle/10665/148114/?sequence=6
4. Tackling Chronic Disease Report 2010. [Internet]. World Economic Forum; Available from: https://www3.weforum.org/docs/WEF_HE_TacklingChronicDisease_Report_2010.pdf
5. Gerteis J, Izrael D, Deitz D, LeRoy L, Ricciardi R, Miller T, et al. Multiple chronic conditions chartbook. Rockville (MD): Agency for Healthcare Research and Quality; 2014. AHRQ Publications No, Q14-0038.[Google Scholar]; 2014.
6. Long-term conditions compendium of Information: 3rd edition. Department of Health, UK; 2012.
7. Megari K. Quality of life in chronic disease patients. Health Psychol Res. 2013 Sep 23;1(3):27.
8. Healthcare expenditure, UK Health Accounts provisional estimates: 2020. Office for National Statistics; 2022.
9. Commission E. Joint Report on Health Care and Long-Term Care Systems and Fiscal Sustainability. Eur Comm Bruss. 2016;
10. Health Care Survey [Internet]. AON Hewitt; 2012. Available from: https://www.aon.com/attachments/human-capital-consulting/2012_Health_Care_Survey_final.pdf
11. Investing in global health: A common objective [Internet]. Wold Health Organisation; 2023. Available from: https://www.who.int/news-room/commentaries/detail/investing-in-global-health--a-common-objective
12. Healthy Living Is the Best Revenge: Findings From the European Prospective Investigation Into Cancer and Nutrition–Potsdam Study. Arch Intern Med. 2009 Aug 10;169(15):1355.
13. Wu J, Wang Y, Tao L, Peng J. Stakeholders in the healthcare service ecosystem. Procedia CIRP. 2019;83:375–9.
14. Kanter RM. Becoming PALs: Pooling, Allying, and Linking Across Companies. Acad Manag Perspect. 1989 Aug;3(3):183–93.
15. How To Achieve The Healthcare Flywheel Effect [Internet]. [cited 2024 Jan 13]. Available from: https://www.forbes.com/sites/forbesbusinesscouncil/2023/11/10/synergy-of-technology-and-services-organizations-the-healthcare-flywheel-effect/#
16. Health promotion glossary. World Health Organization; Geneva; 1998.
17. Health 2020: A European policy framework and strategy for the 21st century. World Health Organization. Regional Office for Europe.World Health Organization; 2013.
18. Wright E, Darer J, Tang X, Thompson J, Tusing L, Fossa A, et al. Sharing Physician Notes Through an Electronic Portal is Associated With Improved Medication Adherence: Quasi-Experimental Study. J Med Internet Res. 2015 Oct 8;17(10):e226.
19. Hibbard JH, Greene J. What The Evidence Shows About Patient Activation: Better Health Outcomes And Care Experiences; Fewer Data On Costs. Health Aff (Millwood). 2013 Feb;32(2):207–14.
20. Edgar WB, Albright KS. Knowledge management activities: Conceptual foundations and research issues. J Inf Sci. 2023 Dec;49(6):1656–76.
21. Wenger, Etienne & McDermott, Richard & Snyder, William. Cultivating Communities of Practice: A Guide to Managing Knowledge. 2002.
22. WHO guideline on self-care interventions for health and well-being, 2022 revision. Geneva. [Internet]. World Health Organization; 2022. Available from: https://www.ncbi.nlm.nih.gov/books/NBK582359/
23. NHS Long Term Plan [Internet]. NHS; Available from: https://www.longtermplan.nhs.uk/wp-content/uploads/2019/08/nhs-long-term-plan-version-1.2.pdf
24. Ranmuthugala G, Plumb JJ, Cunningham FC, Georgiou A, Westbrook JI, Braithwaite J. How and why are communities of practice established in the healthcare sector? A systematic review of the literature. BMC Health Serv Res. 2011 Dec;11(1):273.
25. Lesser EL, Storck J. Communities of practice and organizational performance. IBM Syst J. 2001;40(4):831–41.
26. Prusak L. Knowledge in Organisations [Internet]. 0 ed. Routledge; 2009 [cited 2024 Jan 12]. Available from: https://www.taylorfrancis.com/books/9781136390104
27. Polanyi M. Personal knowledge: towards a post-critical philosophy. Nachdr. Chicago: Univ. of Chicago Press; 2009. 428 p.
28. Gabbay J, le May A. Mindlines: making sense of evidence in practice. Br J Gen Pract J R Coll Gen Pract. 2016 Aug;66(649):402–3.
29. Noar AP, Jeffery HE, Ponniah HS, Jaffer U. The aims and effectiveness of communities of practice in healthcare: A systematic review. PLOS ONE. 2023 Oct 10;18(10):e0292343.
30. Winkelman WJ, Choo CW. Provider‐sponsored virtual communities for chronic patients: improving health outcomes through organizational patient‐centred knowledge management. Health Expect. 2003 Dec;6(4):352–8.
31. Peer Mentoring and Financial Incentives to Improve Glucose Control in African American Veterans. Ann Intern Med. 2012 Mar 20;156(6):I–50.
32. Richardson CR, Buis LR, Janney AW, Goodrich DE, Sen A, Hess ML, et al. An Online Community Improves Adherence in an Internet-Mediated Walking Program. Part 1: Results of a Randomized Controlled Trial. J Med Internet Res. 2010 Dec 17;12(4):e71.
33. Changing patient behavior: the next frontier in healthcare value report. [Internet]. McKinsey & Company; 2012. Available from: https://www.mckinsey.com/industries/healthcare-systems-and-services/our-insights/changing-patient-behavior-the-next-frontier-in-healthcare
34. Cyril S, Smith BJ, Possamai-Inesedy A, Renzaho AMN. Exploring the role of community engagement in improving the health of disadvantaged populations: a systematic review. Glob Health Action. 2015 Dec;8(1):29842.
35. Bild E, Pachana NA. Social prescribing: A narrative review of how community engagement can improve wellbeing in later life. J Community Appl Soc Psychol. 2022 Nov;32(6):1148–215.
36. Oktay LA, Abuelgasim E, Abdelwahed A, Houbby N, Lampridou S, Normahani P, et al. Factors Affecting Engagement in Web-Based Health Care Patient Information: Narrative Review of the Literature. J Med Internet Res. 2021 Sep 23;23(9):e19896.
37. Michie S, Van Stralen MM, West R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement Sci. 2011 Dec;6(1):42.
38. WELLNESS ECONOMY STATISTICS & FACTS [Internet]. Global Wellness Institute; Available from: https://globalwellnessinstitute.org/press-room/statistics-and-facts/
39. Guni A, Normahani P, Davies A, Jaffer U. Harnessing Machine Learning to Personalize Web-Based Health Care Content. J Med Internet Res. 2021 Oct 19;23(10):e25497.
40. Health B. Why the Cambridge Analytica Scandal is Important for Health Data [Internet]. Medium. 2018 [cited 2024 Jan 14]. Available from: https://bowheadhealth.medium.com/why-the-cambridge-analytica-scandal-is-important-for-health-data-db6b9fa1a17e
41. Robinson D, Cybenko G. A Cyber-based Behavioral Model. J Def Model Simul Appl Methodol Technol. 2012 Jul;9(3):195–203.
42. Robinson DJ, Berk VH, Cybenko GV. Online Behavioral Analysis and Modeling Methodology (OBAMM). In: Liu H, Salerno JJ, Young MJ, editors. Social Computing, Behavioral Modeling, and Prediction [Internet]. Boston, MA: Springer US; 2008 [cited 2024 Jan 14]. p. 100–9. Available from: http://link.springer.com/10.1007/978-0-387-77672-9_12
43. Poushpas S, Normahani P, Kisil I, Szubert B, Mandic DP, Jaffer U. Tensor decomposition and machine learning for the detection of arteriovenous fistula stenosis: An initial evaluation. PloS One. 2023;18(7):e0286952.
44. Powezka K, Pettipher A, Hemakom A, Adjei T, Normahani P, Mandic DP, et al. A Pilot Study of Heart Rate Variability Synchrony as a Marker of Intraoperative Surgical Teamwork and Its Correlation to the Length of Procedure. Sensors. 2022 Nov 21;22(22):8998.
45. Powezka K, Adjei T, Von Rosenberg W, Normahani P, Goverdovsky V, Standfield NJ, et al. A pilot study of preoperative heart rate variability predicting pain during local anesthetic varicose vein surgery. J Vasc Surg Venous Lymphat Disord. 2019 May;7(3):382–6.
46. Von Rosenberg W, Chanwimalueang T, Adjei T, Jaffer U, Goverdovsky V, Mandic DP. Resolving Ambiguities in the LF/HF Ratio: LF-HF Scatter Plots for the Categorization of Mental and Physical Stress from HRV. Front Physiol. 2017 Jun 14;8:360.
47. Normahani P, Makwana N, Von Rosenberg W, Syed S, Mandic DP, Goverdovsky V, et al. Self-assessment of surgical ward crisis management using video replay augmented with stress biofeedback. Patient Saf Surg. 2018 Dec;12(1):6.
48. Belle A, Hargraves RH, Najarian K. An Automated Optimal Engagement and Attention Detection System Using Electrocardiogram. Comput Math Methods Med. 2012;2012:1–12.
49. Marketing 101: What is funnel creation? | MarketingSherpa Blog [Internet]. [cited 2024 Jan 14]. Available from: https://sherpablog.marketingsherpa.com/website-and-landing-page-design/marketing-101-funnel-creation/
Knowledge management in Communities of Practice
Knowledge management is defined as ‘the collection of methods related to creating, sharing, using, and managing the knowledge and information’ (30) . Tacit knowledge, first described by Polanyi, the Hungarian-British philosopher in 1966 (31,32), as opposed to explicit knowledge, is very difficult to directly codify and share. It can be communicated through direct observation and imitation as well as through conversations, stories, and metaphors (33).
CoPs are an effective form of knowledge management that have been successfully used in the business sector and increasingly so in healthcare. CoPs are highly effective knowledge transfer vehicles particularly for difficult to communicate tacit knowledge (34) and can foster interdisciplinary care by bringing practitioners from a range of specialities together (35).
We have reviewed CoPs and have reported encouraging outcomes. Interestingly, the most important facilitator reported was strong clinical involvement (36). Online CoPs centred around particular chronic conditions place the patient as a practitioner of their own health. Here, they will be able to learn from both the explicit and tacit knowledge of fellow patients as well as healthcare professionals with expertise in their condition (37).
Randomised controlled trials show how peer support interventions can lead to improved glucose control (38) and increased adherence to lifestyle interventions (39). Furthermore, hospital costs are 24% higher for socially isolated individuals than for socially connected individuals (40). Community participation has been linked to improved real world outcomes particularly in disadvantaged communities (41). Other related concepts such as social prescribing have shown similar benefits (35). Additionally, community participation has been shown to reduce attrition rates in internet mediated health programs (39).
The combination of the knowledge gained (explicit and tacit) as well as social support provided by Health-Shared CoP provides all the ingredients which have been shown to be effective at promoting healthy change. Our group has previously published on factors affecting engagement with online health content. We highlighted many factors relevant to content features including community origin and emotionally relevant, and relevance (42).
Behaviour Change through Communities
The COM-B model of behaviour change frames the different facets required for an individual to change their behaviour (43). They need to have the capability, opportunity, and motivation to generate the desired behaviour. Capability is defined as the psychological and physical requirements to perform the task. Opportunity represents the physical and social factors outside of the individual that make the behaviour possible, and motivation is defined as both reflective and automatic brain activity that energises and directs behaviour.
Health-Shared CoPs will allow patients to find those dealing with similar health related issues to share experiences and problem solve providing them with the capability and motivation to make the behaviour changes they need. As a novel form of social support in their lives, patients will also have the opportunity to engage in healthy behaviours. They will also have trust in the information they are receiving as they will be interacting with trained healthcare professionals with expertise in their particular condition.
Online CoPs are well placed to incorporate many of the intervention techniques for behaviour change namely education through the content they are exposed to on the platform as well as modelling from expert patients who have experience and skill at living with their condition. But also enablement, training and incentivisation.
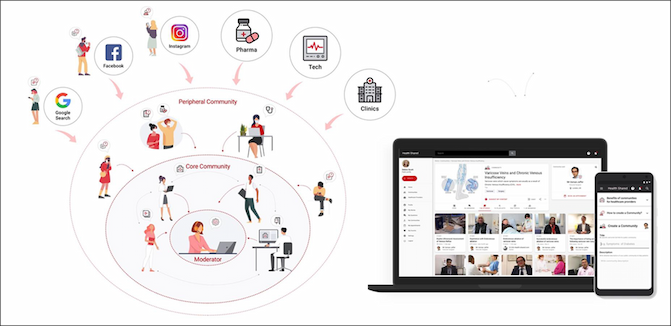
Community Establishment
A Health-Shared CoP includes a core and periphery. The core comprises net content creators and represents all stakeholders in the patient journey - patients, healthcare providers, patient and healthcare provider organisations and industry. The periphery are net content consumers - i.e. people seeking answers. CoP are moderated by human in the lopp AI system to prevent bias and ensure safeguarding.
Figure. Structure of Health-Shared CoP. Core community members comprise of all key stakeholders in the patient journey. Periphery community members consist of people seeking information.
Flagship Communities
Health-Shared will provide national flagship communities for the 15 chronic conditions which account for 80 percent of global health costs.
Local Communities
Health-Shared is seeking to partner with local government and local public health services to provide locally based communities for conditions which have been identified as local priorities. There may be much overlap in the explicit content between the flagship and the local communities. The reason people may wish to join one or more local communities over and above flagship communities is the variation in tacit knowledge which may well be local specific.
Communities as Distributed Autonomous Organisations
Communities should advocate for the needs of the members. Themes relevant to the community are established from thematic analysis of stakeholder interviews, user generated content and user search behaviour. Priorities will be set via polling of the community members. This data will provide a unique and objective view of community needs which can be shared with partners.
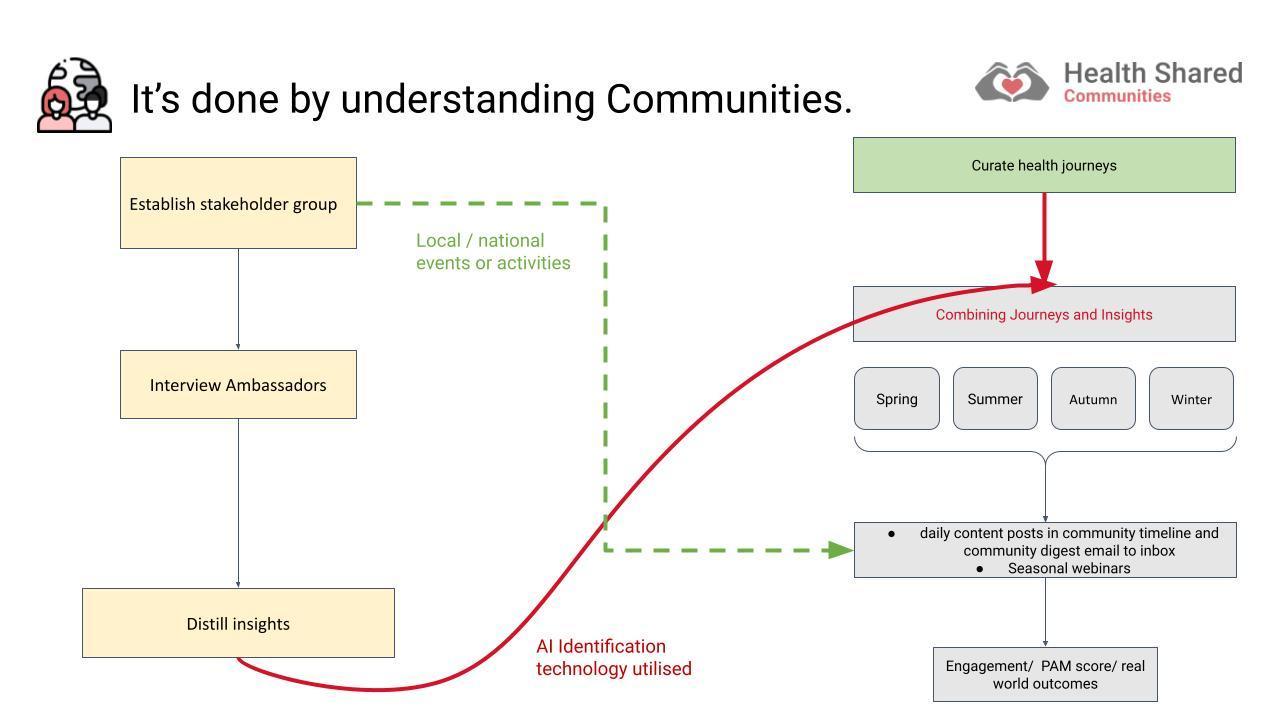
Process for establishing Health-Shared community.
Health-Shared has a unique methodology for establishment of Communities. A protocolised sequence is following:
Figure 3. Process for establishment of communities
Personalisation of content
Content is personalised to users along the Health-Shared concept of light and warmth. We describe communities as camp fires in a dark forest. Users see explicit knowledge from afar (light) and come closer to the campfire (community). When near, they notice the warmth (tacit knowledge) which aligns with themes including: hopes, fears, solutions, strategies, successes and failures.
Figure. Communities purvey light (explicit knowledge) and warmth (tacit knowledge).
Token incentivisation for Community Activism
Tokenising community activism allows Health stakeholders to support users activate. Health-Shared will issue tokens for ‘rewardable’ community activities including:
Partner stakeholders can incentivise community activism and hence activation of community members by increasing numbers of tokens issued for each activity.
Technology Description
The technological backbone of Health-Shared CoP is accomplished by the
use of web 3.0 including 'folksonomies' (tag cloud based, flat
metadata structure for content), complex algorithmic medicine and machine learning. This
allows participants to enhance their self management journey by associating
with tags, themes and personalised content.
Community and Personal feed determinants
Community Feeds
The community feed is determined by the scheduled content programme as set up by the community owner. The schedule should follow the themes extracted from discovery interviews with ambassadors as well as surveys and polls of community members.
With the establishment of a community DAO, this process will be governed by smart contracts. Discovery interviews conducted as the community is set up will create a map of light and warm themes (explicit and tacit).
This theme map will be continually updated in light of user generated content in the community and search terms being used.
Community DAO members will be asked to vote on priority themes for the next season and content will be scheduled based on the DAO priorities.
Personal feed.
A users personal feed is the cumulation of all the communities being followed as well as light and warm (explicit and tacit) tags associated with that users. These tags are derived from the following sources:
Vector DB explicit (light) and tacit (warmth) recommendation system
We have a custom implementation of the Weaviate vector database. The vector database calculates a three dimensional vector as an aggregate of the light and warm (explicit and tacit) tags associated with your profile.
Psychographics engine development.
Psychographics has received negative press in the wake of national election influencing in the Cambridge Analytica scandal (45), however, in its essence, psychographics can be used to present content (both explicit and tacit) in a manner which a user is most likely to be affected by. Others have proposed that cyber based behavioural models are important (46,47).
Health-shared will create a psychographics ML engine to provide an additional layer of personalisation to content being displayed in users personal feeds. We will use user features including personality scores and tags associations and content features including sentiment analysis, content type, length and other off the shelf descriptions as well as novel computer vision approaches that we have previously implemented (48).
Wearable heart rate variability based algorithm to personalise content to individual users psychographic profile.
Health-Shared will refine its psychographics engine with individual user physiological data as well as simple web interaction data. We have previous published in this field (49–52). There are validated signal processing algorithms for detecting attention using ECG heart rate variability (53). We will perform bench research to correlate features of a wrist worn PPG sensor (eg smartwatch) with the ECG heart rate variability detected features of engagement previously reported. We will then incorporate a wrist worn device PPG signal into a psychographics model which will individualise to users.